An important first step in advocating for NPs, midwives, and PAs as abortion providers involves education about the abortion procedure itself. Politicians, regulators, and clinicians are often unaware of the basic training required to become a provider of medication or early aspiration abortion. This lack of understanding can lead to misinformed decisions that unduly restrict training and access.
Although there are multiple types of abortion procedures, this Toolkit focuses on the two methods most commonly used during the first trimester of pregnancy: aspiration and medication.
The vast majority of patients seeking abortion care do so in the first trimester, the time when NPs, midwives, or PAs are most likely to provide abortion care.
“Aspiration” versus “Surgical”: What’s in a Name?
We use the term aspiration abortion when discussing first-trimester abortion care because it more accurately depicts a first-trimester abortion than does surgical abortion. Surgical “implies incision, excision and suturing and is associated with the physician subpopulation of surgeons.”1
Most abortions performed during the first trimester use electric or manual suction to empty the uterus. These simple procedures require only local or oral analgesics and can easily be performed in a primary care setting. Using the term surgical abortion to describe both less invasive aspiration procedures as well as more invasive procedures blurs the boundary between these very different types of procedures.
Not only does the term aspiration abortion clarify important differences between types of abortions, its use can assist efforts to challenge the thinking that only physicians should provide abortion care. Surgeons perform surgery. Aspiration abortion is not surgery. Primary care providers, including NPs, midwives, and PAs, provide a wide range of procedures, including intrauterine device (IUD) insertion, endometrial biopsy, management of early pregnancy loss, and abortion. Use of the term aspiration–rather than surgical–abortion is a small but important step that all of us can take to help de-mystify early abortion techniques.
Medication Abortion
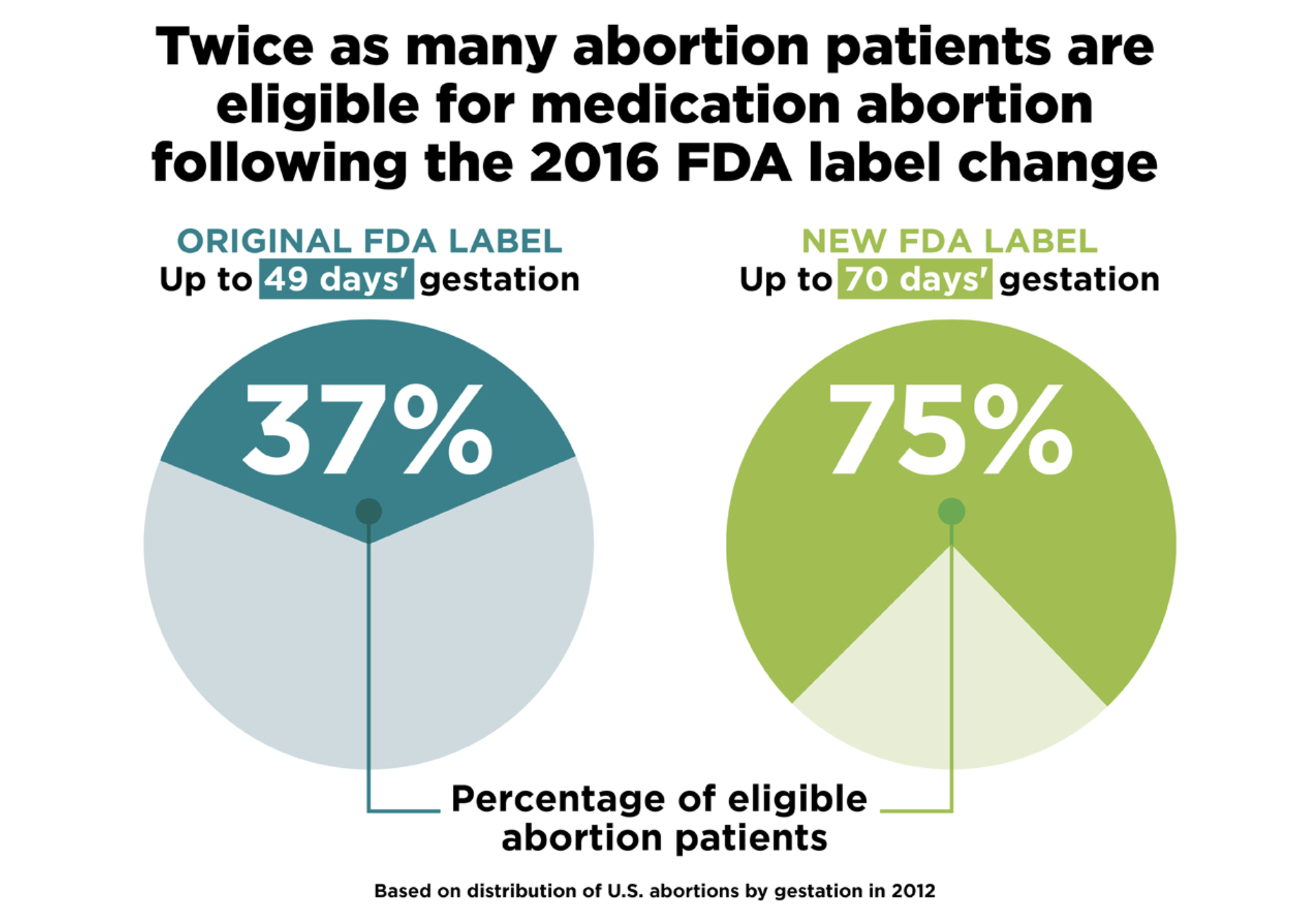
Medication abortion is a method of pharmacologic termination of the early first trimester of pregnancy. Depending on the agent(s), the regimen, and the provider, medication abortion may be initiated as soon as a patient finds out she is pregnant, through 70 days of gestation (via menstrual dating).
Early medical abortion accounts for about 22% of reported abortions in the United States.2
Designed as an educational tool to use with patients considering medication abortion, this short, animated video explains the basics of how medication abortion works and what patients should expect during and after treatment.
Although three medications are available in the U.S.–mifepristone, misoprostol, and methotrexate–methotrexate is rarely used today because of the greater availability and efficacy of regimens using the other drugs. Mifepristone blocks the uptake of progesterone by receptor cells in the uterus. Without this essential hormone, the lining of the uterus begins to break down, and the cervix softens. Misoprostol is a prostaglandin analogue that stimulates uterine contractions and softens the cervix, facilitating uterine emptying.
Medication abortion is an extremely safe and effective procedure. The percentage of cases in which the medications do not successfully terminate the pregnancy and an aspiration procedure is necessary varies depending on the regimen, the gestational age of the pregnancy, and other factors, but in most studies is less than 5% of medication abortions.3
In March 2016, the FDA-approved updated labeling for mifepristone (Mifeprex®), bringing the label in alignment with what had been proven safe and effective and was standard medical practice recommended in the American Congress of Obstetricians and Gynecologists (ACOG) practice bulletin.4
Aspiration Abortion
In the first trimester, abortion can be performed as a simple office procedure using a vacuum aspirator. In aspiration abortion, the cervix usually is gradually stretched with tapered rods. After the cervix is dilated sufficiently, a plastic cannula attached to the suction apparatus is inserted into the uterus. Gentle suction (<60 mmHg) is applied to empty the contents of the uterus. Local anesthesia by means of paracervical and/or intracervical injection is almost universally used, and many clinics offer various other medications for relief of anxiety and pain management. General anesthesia is less commonly used in early abortion but may be offered in some facilities. Aspiration abortion is highly effective, with success rates (complete abortion) at 99%. It is also one of the safest medical procedures and carries minimal risk.

- Weitz TA, Foster A, Ellertson C, Grossman D, and Stewart, FH, “Medical” and “surgical” abortion: rethinking the modifiers, Contraception, 2014, 69(1):77-78. ↵
- Jatlaoui TC, Ewing A, Mandel, MG, et al., Abortion surveillance – United States, 2013, CDC Surveillance Summaries, 2016, 65(12):1-44. ↵
- ACOG, Medical Management of first-trimester abortion, Practice Bulletin, 2014, Reaffirmed 2016, 143. ↵
- ACOG, Medical Management of first-trimester abortion, Practice Bulletin, 2014, Reaffirmed 2016, 143. ↵